A friend recently pointed me towards the First Aid Errata (2007 Edition). Most of the errors were minor typos that would not affect one's learnin. However, I would say about 10% of the errors were significant in terms of content. While I have the 2006 edition, the page was still useful as there will still significant errors in the document that existed in my edition.
One error it noted related to claw hand. The concept of claw-hand had always confused me a little bit, and the mislabeled diagram did not help matters. I was surprised to not find a single good site online that explained the two. This might be more due to my googling skills, but I figured I'd write up what I found.
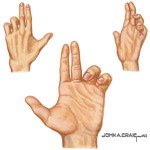 Pope's Blessing / Hand of Benediction
Pope's Blessing / Hand of Benediction
Nerve: Median
Lesion Location: Proximal (near the elbow) [1]
Deficiency: When the patient tries to make a fist, they are unable to flex the index and middle fingers due to loss of lateral lumbrical action, leading to the hand of benediction. The fingers are extended due to unopposed radial nerve action on the finger extensors. I believe the finger will also be adducted due to loss of abducens pollicis brevics (although abducens pollicis longus should still function).
Notes: This lesion is also related to ape hand due to the fact that loss of opponens pollicis means one has an unopposable thumb (like an ape). It seems some also believe the term ape hand refers to the thenar atrophy, but I like the first explanation better.
Lesion Location: Proximal (near the elbow) [1]
Deficiency: When the patient tries to make a fist, they are unable to flex the index and middle fingers due to loss of lateral lumbrical action, leading to the hand of benediction. The fingers are extended due to unopposed radial nerve action on the finger extensors. I believe the finger will also be adducted due to loss of abducens pollicis brevics (although abducens pollicis longus should still function).
Notes: This lesion is also related to ape hand due to the fact that loss of opponens pollicis means one has an unopposable thumb (like an ape). It seems some also believe the term ape hand refers to the thenar atrophy, but I like the first explanation better.

Claw Hand
Nerve: Ulnar
Lesion Location: Medial epicondyle fracture or Guyon Canal entrapment.
Deficiency: There is clawing of the index and middle fingers due to weakness of the ulnar-supplied interossei muscles. [2]
Notes: I think the confusion really starts here since it seems there are two entities discussed: claw hand and ulnar claw hand. The image at right is claw hand as described above. Ulnar claw hand seems to be a late stage of ulnar nerve entrapment in which the ring and little fingers are permanently clawed. It has also been termed "papal claw." I honestly still do not know what someone means when they simply refer to "claw hand."
While I know this post has not been definitive, hopefully it clarified the cause of the confusion here. Clearly, there are still some sources that say pope's blessing / hand of benediction is an ulnar lesion [3 and comments below], but I am still unconvinced. If anyone has a more definitive answer / clarification of what I have written, please comment about it. Thanks!
[1] http://www.studystack.com/studytable-10342
[2]http://forums.studentdoctor.net/showthread.php?goto=lastpost&t=205962[3]http://www.prep4usmle.com/forum/thread/8287
Updated 2008-08-24: I have made the references clearer so you know where the information is coming from.
Updated 2015-12-08: Updated links
my textbooks confirm!
ReplyDeleteThanks for the confirmation!
ReplyDeleteAnother thing that I should have clarified: I think these hand positions have to be elicited in order to be evident. If the lesion is new, the person's hand may look normal until you test their strength or ask them to flex their fingers. However, I am still unclear as to what happens if the person has had the injury for a long time. Anyone have any idea?
Dupuytren's contracture is also sometimes called "claw hand," to add to the confusion :-)
ReplyDeleteIf you have an ulnar lesion, wouldn't IV and V claw instead of the index and middle indicated in the "claw hand" picture by Adam?
ReplyDeleteAm seriously confused now :S!
I think an Ulnar claw hand is a type of claw hand?? And maybe "claw hands" come in lots of flavors eg: different fingers bent - just a speculation based on the figure of the "claw hand" that is shown and looks pretty professional. I am sure based on first aid and high yield that the picture by ADAM is NOT of an ulnar nerve lesion.
ReplyDeleteSo if u're talking about an ulnar claw hand, it is definitely the pinky and ring finger that are permanently flexed.
The difference between the ulnar lesion and a median lesion is that in the median nerve lesion the index and middle finger cannot be flexed when the patient is told to make a fist. However, in the ulnar nerve lesion the pinky and ring finger cannot be UNFLEXED if the patient is told to extend fingers.
Hope I am making some sense....
I think your clarification is correct. I tried to make it clear in the "Notes" that the image is not of an ulnar lesion, but I suppose it is still a bit misleading. I think part of the problem researching this online is that I can't seem to find a good set of illustrations, and I guess I'm too lazy to do an extensive search for Netter's images / better info. If anyone has a link to better images / explanations, please feel free to post them here. It'd be much appreciated.
ReplyDeleteHere in Russian Fed, we use 'gynecologist's hand' for the pope's blessing deformity.....no way you'd confuse that :)
ReplyDeleteIn the process of correcting my FA2007, I googled Pope's Blessing and found your site. Looks like you did right!
ReplyDeleteYou're wrong. I don't mean to sound rude, it's just important that people don't leave this page thinking an ulnar nerve lesion manifests as clawing of the index and middle fingers.
ReplyDeleteUlnar Claw explained
Ulnar lesions (particularly at the wrist) result in hyper-extension of the MCP joints and flexion at the IP joints of the 4th and 5th digits (ring and pinky), an "Ulnar Claw". This is due to the actions of the extrinsic muscles of finger movement (long flexors and extensors of the forearm) being unopposed by the non-functioning medial two lumbricals which were under ulnar innervation. To try understand this think of what it is the lumbricals do. They flex the MCP joint and extend IP joints (the so-called "Writer's Upstroke"), so it makes sense that the loss of the lumbricals will manifest as the opposite. The index and middle fingers remain normal because the lateral two lumbricals are under median nerve control. The deformity will become most obvious when the patient is asked to straighten their fingers. The interossei are involved in ABduction and ADduction of the fingers and play no role in clawing.
Ulnar Paradox. The above is an explanation of distal ulnar nerve damage, where only the intrinsic nerves of the hand are effected. If the ulnar nerve is damaged at the elbow we also loose the function of the medial half of Flexor Digitorum Profundus. This results in less "clawing" of the 4th and 5th phalanges because of less flexion being exerted on them. This means that even though more muscles are lost with more proximal damage to the nerve, the manifestation is less severe=The Ulnar paradox.
Median nerve lesions at the wrist can cause clawing of the index and middle finger such as seen in that second photo, and for the very same reason that ulnar clawing happens(loss of the relevant lumbricals and unopposed action of forearm flexors and extensors).
Combined distal median-ulnar lesions will cause clawing of all 4 fingers.
Sorry for the long post, but it took me ages to straighten out in my head, so I though I'd help others get there faster! Feel free to put this up as a stand alone blog post. I think the current post needs to be fixed to avoid any more confusion on this one! :)
Sources:
Gray's Anatomy for students
Illustrated Clinical Anatomy
www.wheelessonline.com/ortho/ulnar_nerve
medscape.com/viewarticle/573269_6
And a million other places.. :)
dear sir i am not a medical student.
Deletei am suffering from above problem from last 3 years as shown in figure 1 above. is there any treatment available for the above problem.
i met an accident and got lateral condyle fracture in my right hand. the outer bone piece has been removed from elbow.
now i am unable to club my fingers as will as there is claw on the hand.
please reply me @ harikrishans@gmail.com
regards
harikrishan
Hmm, well, that WAS rude. If it were clarified in a "million other places," then why does everything I've seen refer to median and ulnar nerve injury for Pope's blessing and claw hand, respectively?
ReplyDeletePerhaps my million places comment was misleading. I meant it to highlight just how hard it is to find the correct explanation to the ulnar nerve question (one needs to sift through a million incorrect sites to do it). Unfortunately the rudeness is unavoidable, as any comment contradicting someone's blog will come across that way. However a lot of medical students will come across this page trying to straighten this issue out in there head (as I did). The correction needed to be made, as it was done in others' comments also.
ReplyDeleteI forgot to add a bit on Dupuytren's contracture in my first post, so here it is.
Dupuytren's contracture is a deformity of the hand due to thickening of the palmar aponeurosis with resultant fibrosis and eventual contracture of the medial two fingers (ring and pinky). Presenting as a small hard nodule in the base of the ring finger, it tends to affect the ring and little finger as puckering and adherence of the palmar aponeurosis to the skin. Eventually both the MCP and IP joints of the ring and little finger become permanently flexed. (cf. ulnar claw where the MCP joints are hyper-extended)
Source:
McMinn's Clinical Atlas of Human Anatomy 6thEd (copy and pasted from attached DVD)
I appreciate the additional information, but I think the point of my post originally was that the information WAS so confusing. If there were one definitive source, no one would end on this page, right?
ReplyDeleteBut, yea, Bean/Adrian, I agree with you. That's how I originally conceived of the various lesions. However, FA prior to 2007 I think was incorrect, as were several other texts, hence the confusion. I tried finding the best sources I could, but there was surprisingly little out there, so I wrote my post. Perhaps I'll do an updated post to clarify things.
:) trust me, I feel your pain on trying to find the answer to this one! Different answers in different books (or even between editions) really doesn't help either! I've put the explanation up on wikipedia too, so hopefully that'll help people in the future. Cool blog, keep it up!
ReplyDeleteThanks for doing that. I edit Wikipedia too, but only when I see errors that I know are 100% wrong. I wasn't sure enough about this one to do that (heh, obviously).
ReplyDeleteokay, i read through everything on this entry.
ReplyDeleteBut can i get a clarification?
So ulnar nerve lesion, no matter how you cut it, will give you claw hand of the ring and pinky finger?
And median nerve lesion, will give you hyperextensive index and middle? And i guess, possibly clawing as well????
Thanks!!!
An ulnar nerve lesion will give you the clawing of the 4th and 5th digits, provided it's both severe enough and proximal enough (i.e. wrist or above) to cause paralysis of the muscles in the hand, yes. If it is at the level of the elbow or above the clawing will still happen, but it won't be as severe (the paradox).
ReplyDeleteThe median nerve lesion can give the same appearance (hyper-extension of the MCP joints and flexion at the IP joints) in the index and middle. Information on this one isn't as easy to come by though, perhaps because significant lesions to the nerve aren't as common due to it's route down the middle of the upper limb. Be sure not to confuse this situation with carpal tunnel syndrome. I haven't seen anywhere saying that you'll get clawing with that.
Note, this is how things will appear in a relaxed hand. Things get more complicated when you start talking about how the hand appears when the patient is asked to make a fist (Which is probably the source of all the problems on this issue anyway). I'm afraid I don't have the research done on this one to say what happens for sure, and I don't want to guess in case I'm wrong. Hope it helps.
okay, so i think your information is wrong... The ulnar claw will mean that you are hyper-extended at your ring and lil finger at the mcp joints but flexed at the dip and pip (flexed because the median nerve isn't injured here..just the ulnar and the ulnar only controls the flexing of the metacarpalphalangeal joints at the ring and lil finger and when not working, it is extended at that point)... and w/the median nerve problem, your hand is in fact in the benedict/pope formation because the median nerve controls pip and dip and since the median nerve can't help you flex them, they remain straight...
ReplyDeleteIt may be too obvious, but before getting too carried away with theoretical lesions in different areas and what they would look, it might be worth considering what lesions you could realistically see at various levels. When I was doing a neurosurgery rotation we had a patient with a completely severed median nerve at the wrist, which had happened accidently on a broken glass. Nearly of the flexor tendons were severed as well. Obviously there wasn't 'typical' posturing.
ReplyDeleteActually this is incorrect. The picture at the top shows a hand with the medial two digits flexed and listed as the cause is the median nerve. This is incorrect as the ulnar nerve innervates the medial lumbricals (which is primarily responsible for flexion of the medial two digits via extensor hoods) as well as the flexor carpi ulnaris and 1/2 of the flexor digitorum profundus. It would be impossible for the median nerve to cause what is depicted as an ulnar claw or "pope's hand". That is only caused by trauma or transection of the ulnar nerve; typically below the medial epicondyle of the humerus or at the medial border of the wrist. Hope this helps.
ReplyDeletejust wanted to say thanks for this!!! I'm a PA student and I have a test tomorrow over this all (pray I do good). Helped a load. Thanks
ReplyDeleteGlad to hear it. Hopefully it didn't confuse you too much. Good luck on your test!
ReplyDeletelol...It cleared up a few things my notes/book/Wikipedia wasn't able to.
ReplyDeleteTest didn't go too bad...hopefully.
Any hints on how to digest all the anatomy? It seems a little overwhelming needless to say.
This comment has been removed by the author.
ReplyDeleteI think I see where the confusion is coming in. I agree with Bean/Adrian about the clawing.
ReplyDeleteHowever, seperation of the median nerve proximal to the elbow could produce something that resembled an ulnar nerve claw, but only when the patient is trying to make a fist.
Median nerve seperation above the elbow would result in loss of innervation to the flexor digitorum sperficialis, the lateral half of the flexor digitorum profundus, the lateral 2 lumbricals, and the thenar emminance (among others).
Therefore, you would not get a median claw (because your flexors don't work) and your hand would look pretty normal when relaxed. Now when you try to make a fist you will not be able to flex your lateral two fingers and you will have a symian hand (unopposable thumb). However, your medial two fingers will flex due to the action of the medial two lumbricals and the medial half of the flexor digitorum profundus.
Thus, it may resemble an ulnar claw, but it is not the same thing because ulnar clawing is passive when the hand is relaxed, but a proximal median nerve lesion would only manifest in this way during an attempt to make a fist.
Hope that makes sense. please correct me if I'm wrong 'cause I just logick'd it through. Thus, I have no sources.
Good page, very helpful.
ReplyDeleteHowever, it seems that "benediction hand" looks the same as "ulnar claw", but "benediction hand" is often categorized under median nerve impairment. Oy vey!
Hi =) I agree with Bean & Adrian & Will. Maybe I could help make things simpler.
ReplyDeleteMedian nerve innervates lumbricals 1 & 2. Ulnar nerve innervates Lumbricals 3 & 4. Action of lumbricals: Flex metacarpophalangeal joints and extend interphalangeal joints.
So, in median nerve injury, you will not be able to flex the metacarpophalangeal joints and extend interphalangeal joints of the 2nd & 3rd digits (lumbricals 1 & 2), but rather have the opposite: extension of the metacarpophalangeal joints and flexion of the interphalangeal joints of the 2nd & 3rd digits. This is the claw hand or more specifically median claw hand.
In ulnar nerve injury, you will not be able to flex the metacarpophalangeal joints and extend interphalangeal joints of the 4th & 5th digits (lumbricals 3 & 4), but rather have the opposite: extension of the metacarpophalangeal joints and flexion of the interphalangeal joints of the 4th & 5th digits. This is the Pope's Blessing or Hand of Benediction or ulnar claw hand.
Hi,
ReplyDeleteI actually suffered from this "Pope's Hand" for about a year. I was working out pretty strong and one night something went wrong in my bicep & elbow, it was the worst pain I ever felt. Almost like a "charlie horse" at Maximum capacity. Eventually the pain subdued, but the next morning, my hand was stuck in the 'pope position'. So much so the doctor joked about it and actually called it that. I had all kinds of test run, but they couldn't figure it out. So I just quit using my hand, only making minimum movements & eventually it went back to normal. however, it still gets numb from time to time and even if I try to work it out a little the pain & tingle comes right back & i stop. So from reading all the text. I guess the difference is one is permament & one is temporary.
As much as I appreciate this post, SDN is NOT a reference source. Nor is usmleprep or whatever.
ReplyDeleteUpToDate, Netter's, Musculoskeletal textbooks. Let's get to the heart of this. Thanks for the post, Bean.
http://books.google.com/books?id=ktEPPiLeiWoC&pg=PA227&lpg=PA227&dq=popes+blessing+nerve&source=web&ots=DJ6XDYRklu&sig=tLctfJ4fQ6YCuf92vZgRVM5WXWs&hl=en&ei=RxyWSb3EHomQtQPw6Y18&sa=X&oi=book_result&resnum=5&ct=result
ReplyDeleteYeah, you don't have it completely right.
ReplyDeleteComment by Bean is pretty on the money, but here's the thing.
First, clawing has to do with what happens to the hand when the patient is asked to straighten/extend his fingers.
If the ulnar nerve is damaged then you get ulnar claw (2nd/3rd digits straight, 4th/5th digits extended at the MCP and flexed at the PIP and DIP). This is due to loss of the ulnar innervated lumbricals that leave the radial extensors unnopposed.
If the median nerve is damaged, then you get the same deformity - but only with the 2nd & 3rd digits instead. This is median claw.
If the patient is asked to make a fist, and said patient has median nerve damage then you get the hand of benediciton (2nd/3rd digits slightly arched, 4th/5th digits completely flexed). This is due to loss of the FOREARM flexors innervated be the median nerve.
The confusion stems from the fact that the Hand of Benediction/ Pope's Blessing looks very similar to Ulnar Claw... The similarity is only superficial though, the mechanism resulting in the deformity is different.
So Pope's blessing refers to a PROXIMAL median nerve injury and is seen upon MAKING A FIST.
Claw hand, without further descriptive modifiers, refers to a PROXIMAL unlar nerve injury and is seen upon MAKING A FIST.
An ULNAR CLAW is DISTAL ulnar nerve damage demonstrated upon finger EXTENSIOM.
Likewise, a MEDIAN CLAW is DISTAL medial nerve damage demonstrated upon finger EXTENSION.
So there's 4 diffent hands, one for proximal and distal nerve injury of both ulnar and median nerve. 3 have the word claw in there name and 2 of the hands resemble each for dissimilar reasons... hence, why it's so confusing and generally poorly understood.
Ok, so median claw is the same as ape hand???? :-)
ReplyDeleteI'm using First Aid 2009 right now (Step 1 in three days...FML), and it's terrible on this subject. It says a distal lesion of the median nerve (caused by carpal tunnel or dislocated lunate) gives a sign of Pope's blessing. On the next page, it says a distal median nerve lesion gives you clawing of 2nd and 3rd digits. On that same page, under a picture of a hand giving Pope's blessing, it says "Claw hand of 4th and 5th digits ('Pope's Blessing'); distal ulnar nerve lesion." The naming system described two posts above works for me, but it'd be nice to know if that naming system for these signs is widely accepted.
ReplyDeleteI am physiotherapist from Croatia.I hope this will be helpful.
ReplyDeleteI had patient biten by snake on median side of the forearm and ulnar nerve were damaged.
It was clawing of the 4th and 5th digits.Another one was alcoholist which broke window with forearm and damaged ulnar nerve.This is ofen in alcoholists.They also often sleep soundly lying on their hand and then radial nerve can be damaged(this is called saturday night disease-hanging hand).
Another one were patient which had median nerve injuru caused by shrapnel,so median nerve lesion give hyper-extension of the MCP joints and flexion at the IP joints of the index and middle.I hope this was helpful.
Of course, I can not exactly say was it proximal or distal ulnar lesion in first and second case.Same with the median.But Popes blessing is ulnar lesion, and median nerve gives ape hand.But,if you had distal ulnar laesion you will have clawing of the 4th and 5th digits,in distal medial lesion you will have give hyper-extension of the MCP joints and flexion at the IP joints of the index and middle,BUT mixed with passive,"seamlessly" clawing of 4th and 5th digits,because median inervates half of a 4th finger together with ulnar.In this case 4th finger will be drawn in flexion a little,and 5th finger will be indrawn in flexion barely noticeably.In mixed ulnar-median injury-we have hyper-extension of the MCP joints and flexion at the IP joints of the index and middle together with clawing of the 4th and 5th digits.
ReplyDeletedammit, FA should just draw out what they mean! This thread has been going on for 2 years!
ReplyDeleteThe post on 4/03/2009 is 100% correct. VERY important to notice the subtleties between "claw" and "pope's blessing".
ReplyDeletePope's blessing will have slightly arched index and middle finger and completely flexed 4th and 5th fingers. This is the result when asking the pt to make a fist. MEDIAN NERVE PROBLEM
Ulnar claw will have completely extended index and middle and 4th and 5th will be partially flexed. This will result when asking a pt to extend all of their fingers. ULNAR NERVE PROBLEM
Also, if you ask a person with a median nerve issue to extend fingers all of their fingers (as you would ask to produce the ulnar claw finding in someone with an ulnar issue), they will have the "median claw" finding: 4th and 5th fingers fully extended, but the index and middle fingers partially flexed (because they cannot extend).
-d
note that you examine claw hand by asking the patient to open the hand and extend the fingers.
ReplyDeleteulnar nerve innervates 3rd and 4th lumbrical, that causes flexion of 4th and 5th MCP and extention of 4th and 5th PIP and DIP.
http://emedicine.medscape.com/article/1243669-overview
(Ulnar nerve injury
Ulnar nerve lacerations are commonly referred to as high or low to reflect whether the injury affects extrinsic and intrinsic muscles.3,5,6
High ulnar nerve injury results in paralysis of the flexor carpi ulnaris and the ulnar half of the flexor FDP muscles, generally FDP III-V. The distal phalanges of the fourth and fifth fingers cannot flex. Because the FDP motor units have a common origin, some weak flexion of the fourth and fifth fingers may be possible, even if the ulnar half is supplied by the ulnar nerve. An attempt to flex the wrist results in radial deviation due to paralysis of the flexor carpi ulnaris.
All 7 interosseous muscles, the third and fourth lumbrical muscles, the adductor pollicis muscle, generally also one head of FPB, and all 3 hypothenar muscles (flexor digiti minimi brevis, abductor digiti minimi, and opponens digiti minimi) are paralyzed. The patient cannot adduct or abduct the fingers. If the examiner places a piece of paper between the patient's fingers he or she cannot hold it when the examiner pulls the paper away.
The MCP joints are hyperextended, and the IP joints are flexed. These changes are more obvious at the ring and little fingers, because the first and second lumbrical muscles are not paralyzed. This condition is called a claw-hand deformity . The thumb can weakly adduct through the extensor pollicis longus. The patient can pinch and hold a paper between the thumb and index finger by strongly flexing the IP joint with the flexor pollicis longus. The combination of strong IP and weak MCP flexion called the Froment sign.
Ulnar nerve injury at the wrist spares the flexor carpi ulnaris and the medial half of the FDP muscles. The patient can flex the wrist and all the distal IP (DIP) joints. However, all intrinsic muscles innervated by the ulnar nerve are paralyzed, and both the clawhand deformity and the Froment sign are prominent (see Image 2).)
Thank you all for your valuable contributions.
ReplyDeleteOne point I would like to clarify is that both Ulnar and Median lesions could cause a "Pope's blessing". I elaborate below:
Simply put, the ulnar nerve controls the pinky and ring fingers.
The median nerve controls the index and middle fingers.
(Generally speaking although not 100% accurate)
A Pope's blessing could arise from Not being able to "flex" the index and middle on a command of fisting(Flexion of fingers) or Not being able to extend the pinky and ring on a command of Relaxation (Extension of fingers).
That's a very good point Mohamad. Thanks for pointing it out.
ReplyDeleteLast's Anatomy confirms. I'm tired now so here's the copy and paste from my own wikified notes:
ReplyDeleteClaw hand (sometimes called ulnar claw to distinguish it from other types of claw hand) usually refers to the appearance of the hand in a low ulnar nerve lesion. The affected hand:
is hyperextended at the MCP joints of the 4th and 5th fingers, due to paralysis of the interossei and lumbricals that flex the MCP joint and the unopposed action of extensor digitorum;
is flexed at the interphalangeal joints of the 4th and 5th fingers, due to paralysis of the interossei and lumbricals that extend the IP joints and the unopposed action of flexor digitorum profundus.
Other names
Claw hand is sometimes called hand of benediction/benediction hand. This term is best avoided as it also refers to the claw hand of a median nerve lesion, in which the index finger is typically extended while the 3rd-5th fingers are flexed.
Source: Sinnatamby C, editor. Last's Anatomy. 11th ed. Edinburgh: Elsevier/Churchill Livingstone; 2006.
beautiful a key to succeed in medical school...while confusing the very basic fundamentals...hey Neanderthal check out ulnar and median innervation of lumbricals (lumbricals extend not flex) ulnar is 4th and 5th and median for 2nd and 3rd... that will create exactly the opposite signs. check the first aid 2010 page number 371. god damn confuser makers
ReplyDeleteThanks a lot! Finally it is clear to me!
ReplyDeleteHere's my take on it: http://i.imgur.com/DnyyR.png
ReplyDeleteThe way I look at it is in terms of the nerve, location, and impaired action.
Let me know if there are any errors in the diagram or confusion. Hopefully I got it right lol
Hope it helps!
Right on the money here! Thanks!
DeleteAll depends on whether the nerve lesion is proximal (elbow) or distal (wrist)
ReplyDeleteProximal: inability to flex (due to loss of FDP innervation)
2&3: median n. injury
4&5: ulnar n injury
Distal: inability to extend (FDP innervation not lost)
2&3: median n injury
4&5: ulnar n injury